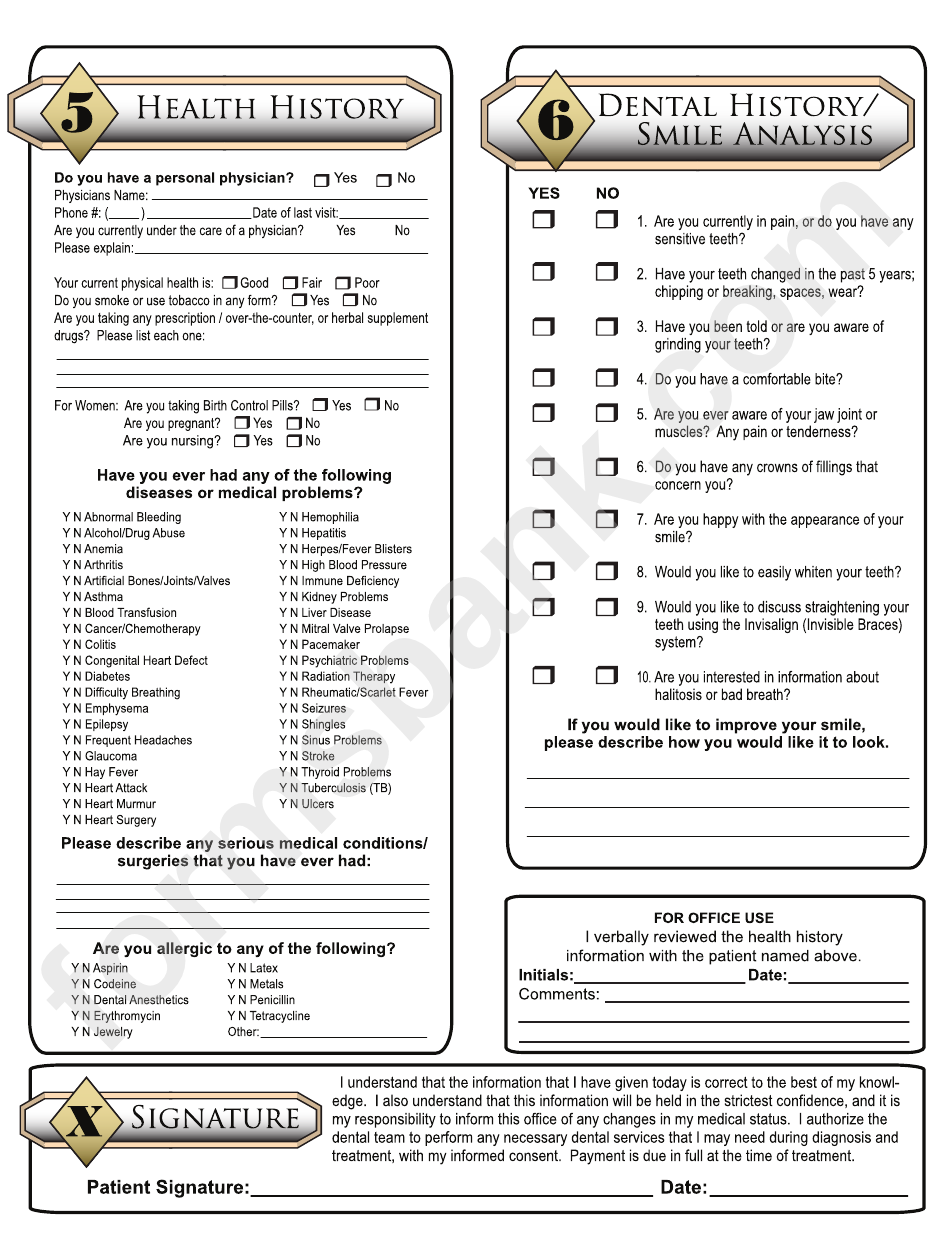
Printable Medical History Update Form For Dental Office - This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. Complete it to ensure accurate healthcare and treatment. Prefered method of contact (select all that. Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your. This form collects updated medical and dental history from patients. To ensure the highest quality of healthcare, we ask that you complete this patient update. To ensure the highest quality of healthcare, we ask that you complete this patient update form. This office will collect, use and disclose information about you for the following purposes, including: What was done at that time? Your response to indicate if you have or have not had any of the following diseases or problems.
This office will collect, use and disclose information about you for the following purposes, including: Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your. This form collects updated medical and dental history from patients. Date of your last dental exam: Your response to indicate if you have or have not had any of the following diseases or problems. To ensure the highest quality of healthcare, we ask that you complete this patient update form. Complete it to ensure accurate healthcare and treatment. Prefered method of contact (select all that. To ensure the highest quality of healthcare, we ask that you complete this patient update. • to deliver safe and efficient patient care and to.
To ensure the highest quality of healthcare, we ask that you complete this patient update. Your response to indicate if you have or have not had any of the following diseases or problems. This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. • to deliver safe and efficient patient care and to. This office will collect, use and disclose information about you for the following purposes, including: This form collects updated medical and dental history from patients. Complete it to ensure accurate healthcare and treatment. Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your. Prefered method of contact (select all that. To ensure the highest quality of healthcare, we ask that you complete this patient update form.
Medical History Forms 10 Free PDF Printables Printablee
What was done at that time? • to deliver safe and efficient patient care and to. To ensure the highest quality of healthcare, we ask that you complete this patient update. This office will collect, use and disclose information about you for the following purposes, including: Complete it to ensure accurate healthcare and treatment.
Editable Dental Medical History Update Form Template Word Sample
Complete it to ensure accurate healthcare and treatment. This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. What was done at that time? This office will collect, use and disclose information about you for the following purposes, including: To ensure the highest quality of healthcare, we ask that.
40 Dental Medical History form Template Markmeckler Template Design
• to deliver safe and efficient patient care and to. To ensure the highest quality of healthcare, we ask that you complete this patient update. Prefered method of contact (select all that. Complete it to ensure accurate healthcare and treatment. This office will collect, use and disclose information about you for the following purposes, including:
Medical History Form For Dental Office templates free printable
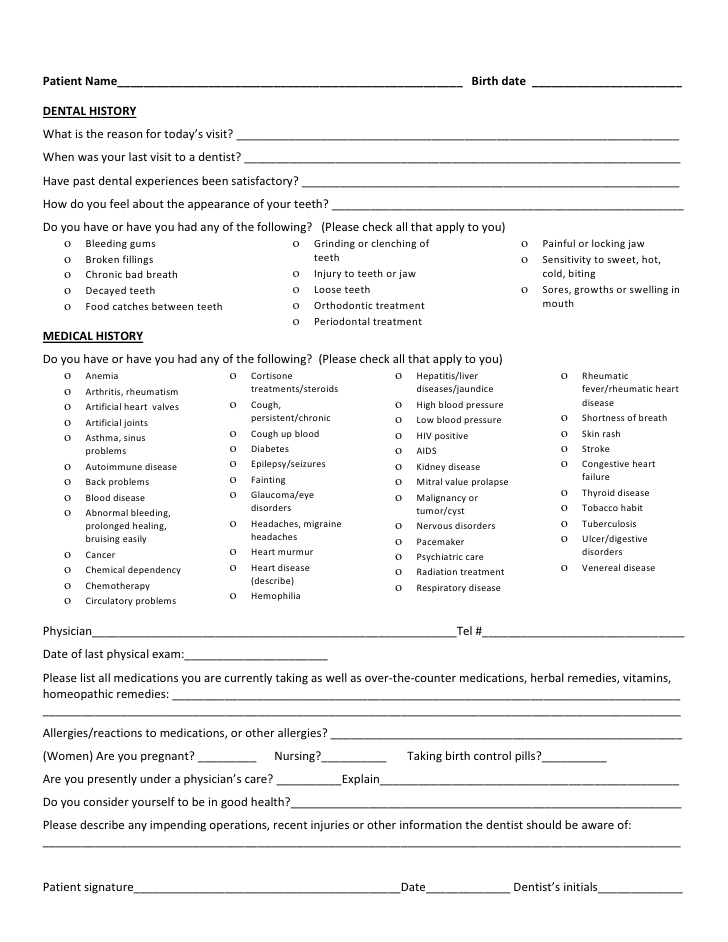
This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. To ensure the highest quality of healthcare, we ask that you complete this patient update form. Date of your last dental exam: Use the 2021 edition of the ada patient dental and medical health history information form to collect.
Dental History Form printable pdf download
Date of your last dental exam: Your response to indicate if you have or have not had any of the following diseases or problems. To ensure the highest quality of healthcare, we ask that you complete this patient update form. Prefered method of contact (select all that. Use the 2021 edition of the ada patient dental and medical health history.
Dental Medical History Form Templates at
Date of your last dental exam: This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. To ensure the highest quality of healthcare, we ask that you complete this patient update form. • to deliver safe and efficient patient care and to. To ensure the highest quality of healthcare,.
Medical History Form For Dental Office templates free printable
This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. What was done at that time? This office will collect, use and disclose information about you for the following purposes, including: Date of your last dental exam: Complete it to ensure accurate healthcare and treatment.
Printable Medical History Update Form For Dental Office Printable
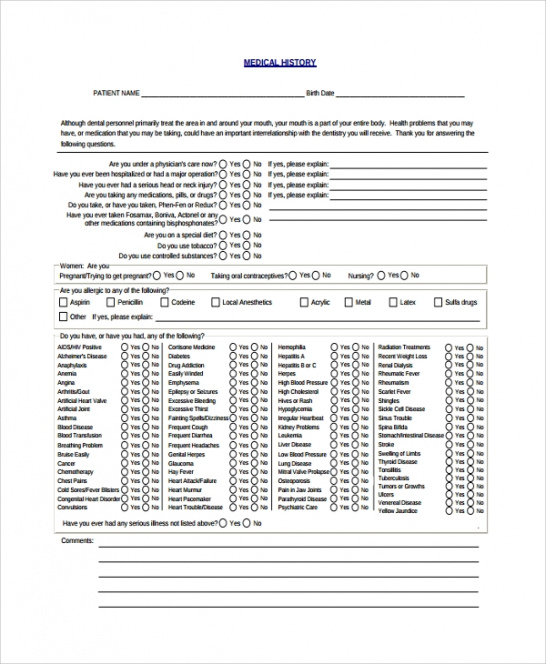
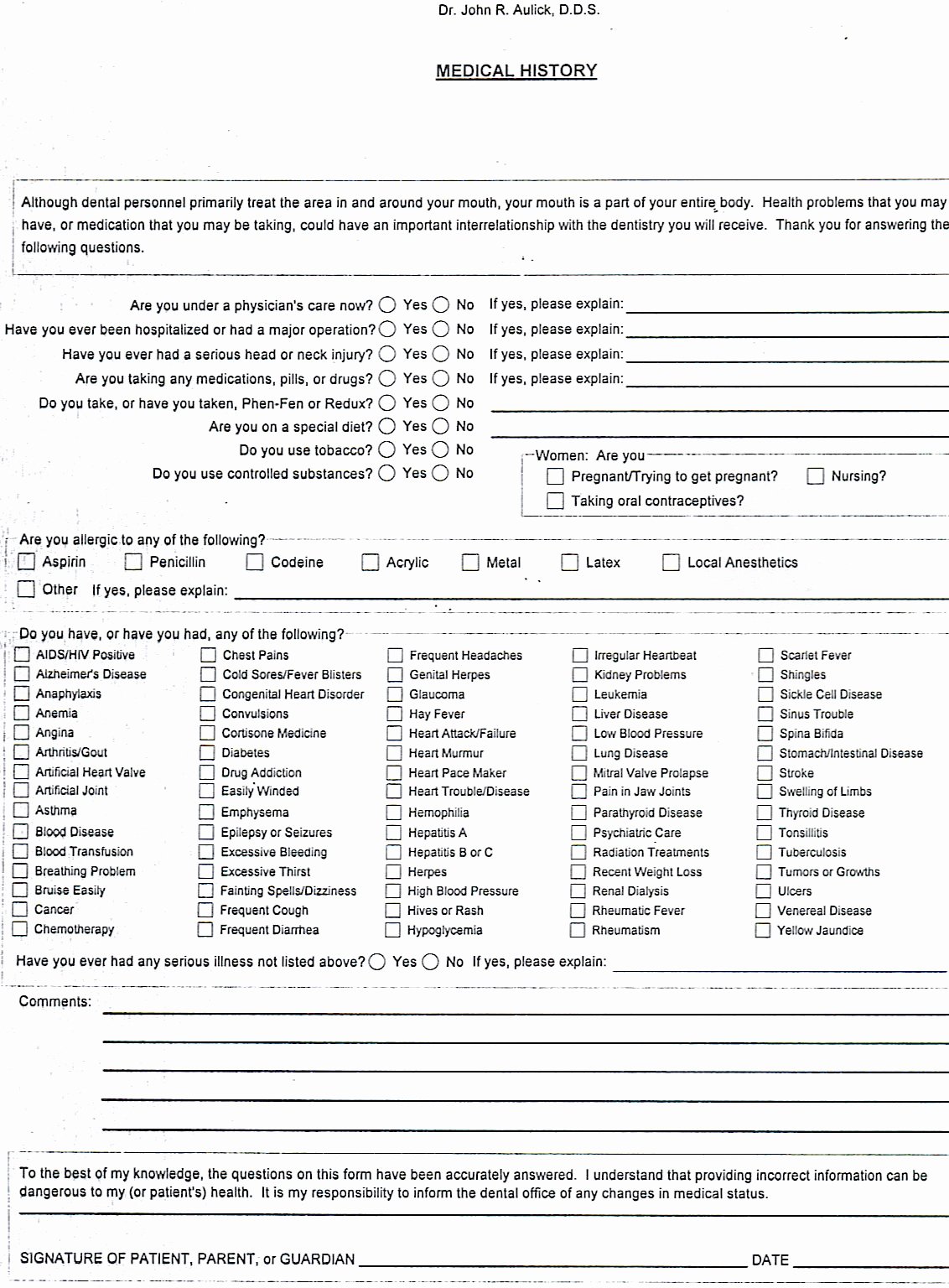
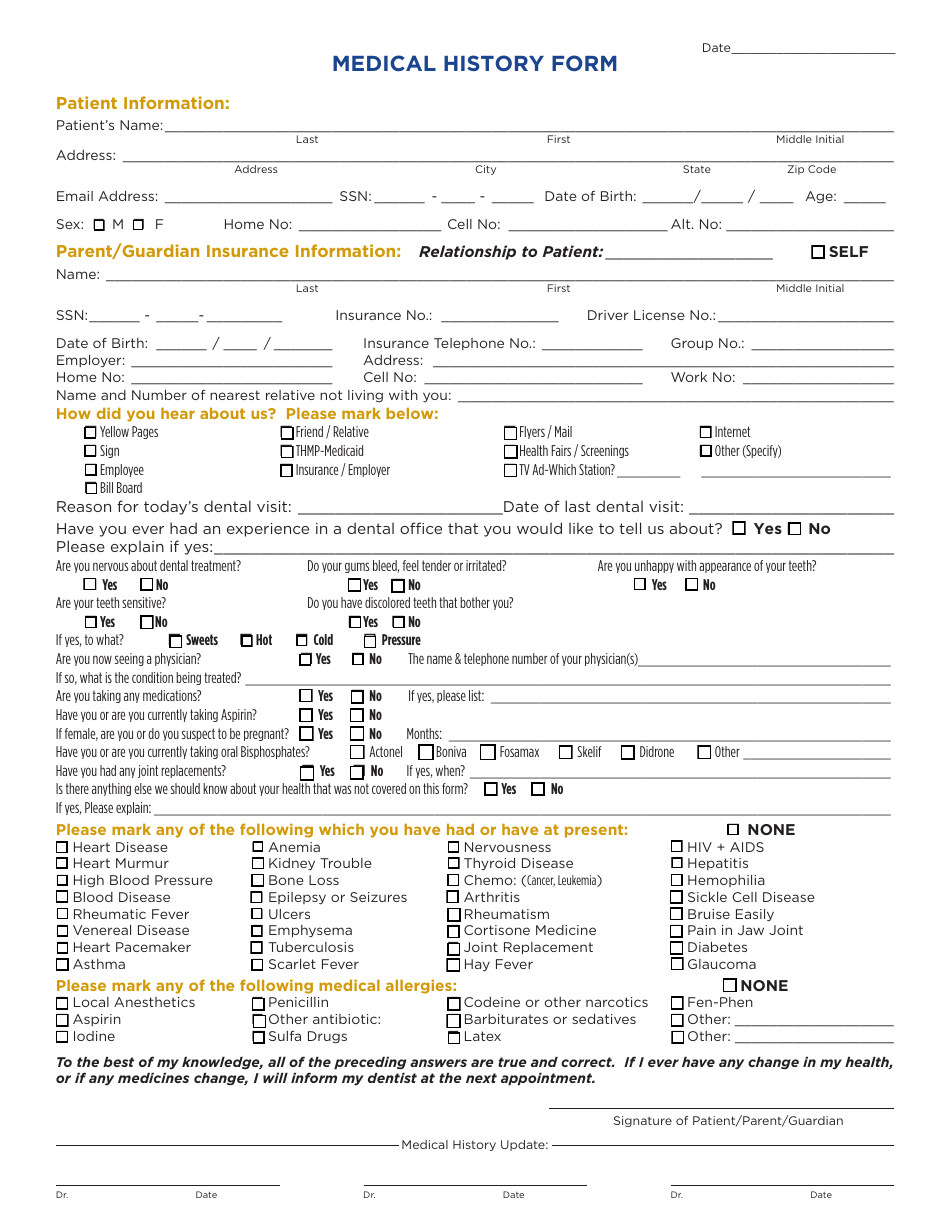
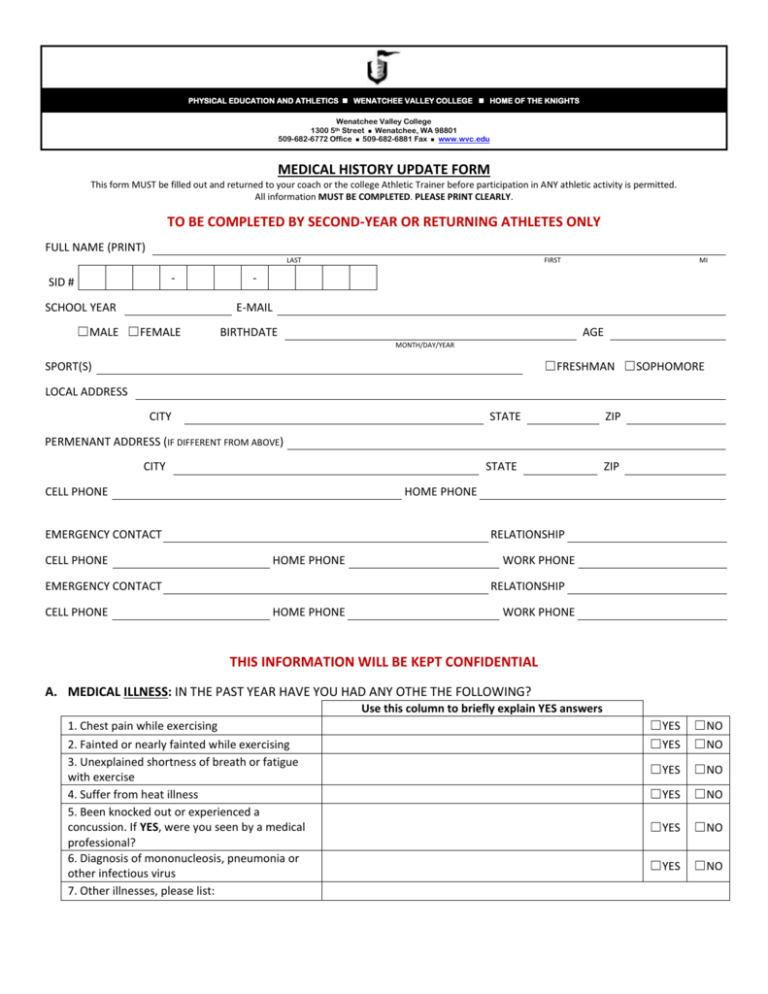
Your response to indicate if you have or have not had any of the following diseases or problems. This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. What was done at that time? Use the 2021 edition of the ada patient dental and medical health history information form.
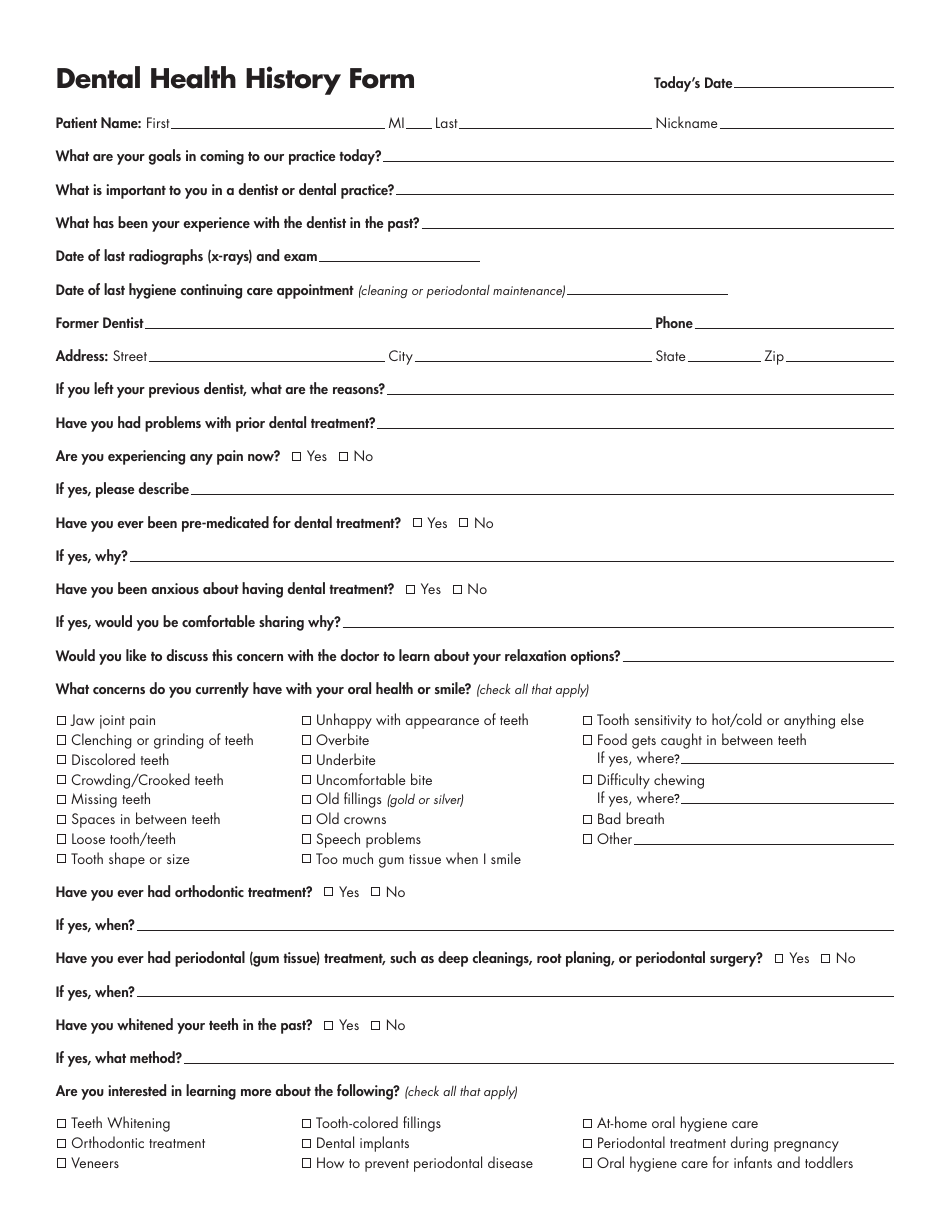
Dental Health History Form Fill Out, Sign Online and Download PDF
This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. What was done at that time? To ensure the highest quality of healthcare, we ask that you complete this patient update. • to deliver safe and efficient patient care and to. Prefered method of contact (select all that.
Printable Medical History Update Form For Dental Office Printable
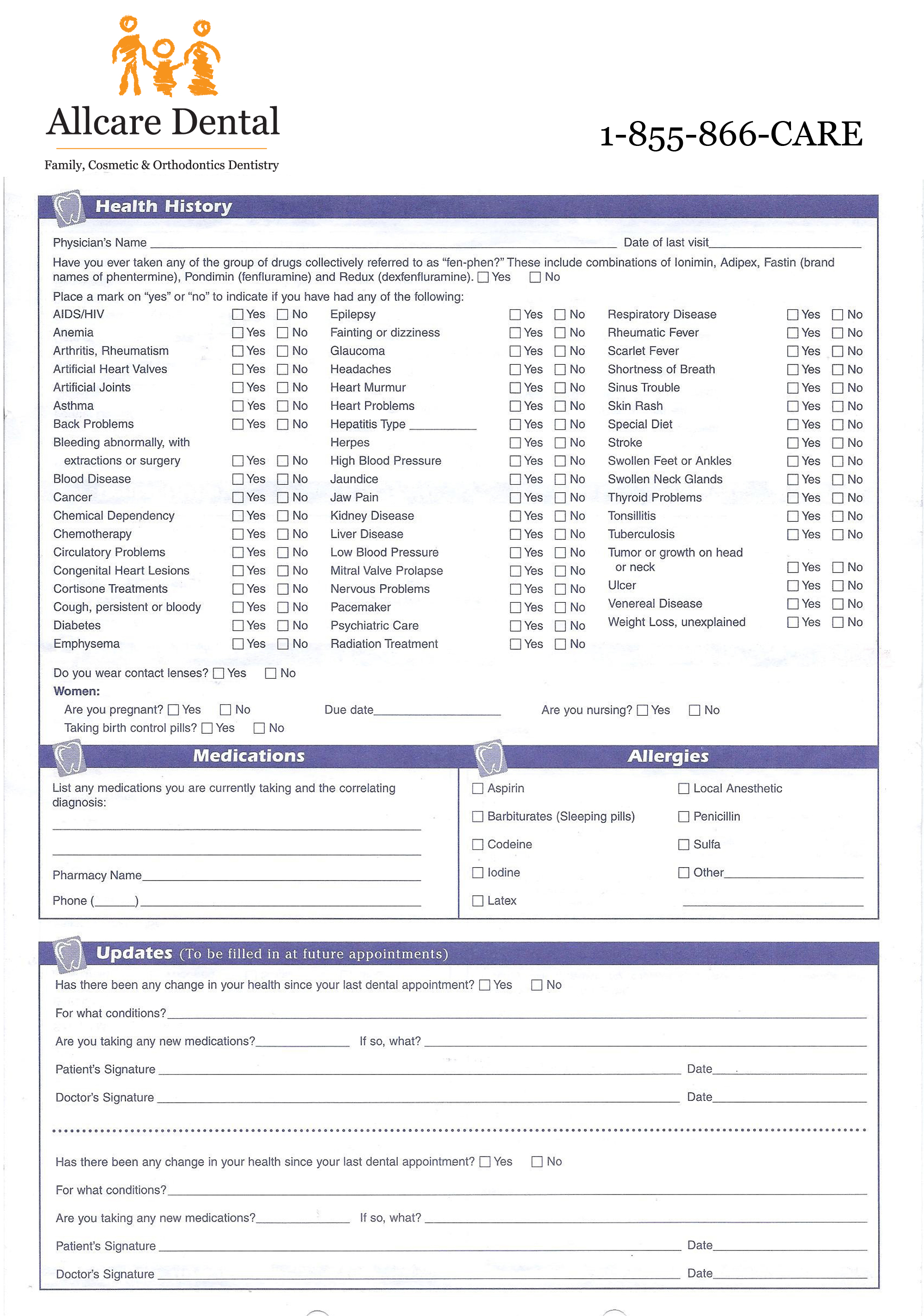
This form collects updated medical and dental history from patients. Date of your last dental exam: Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your. • to deliver safe and efficient patient care and to. This office will collect, use and disclose information about you.
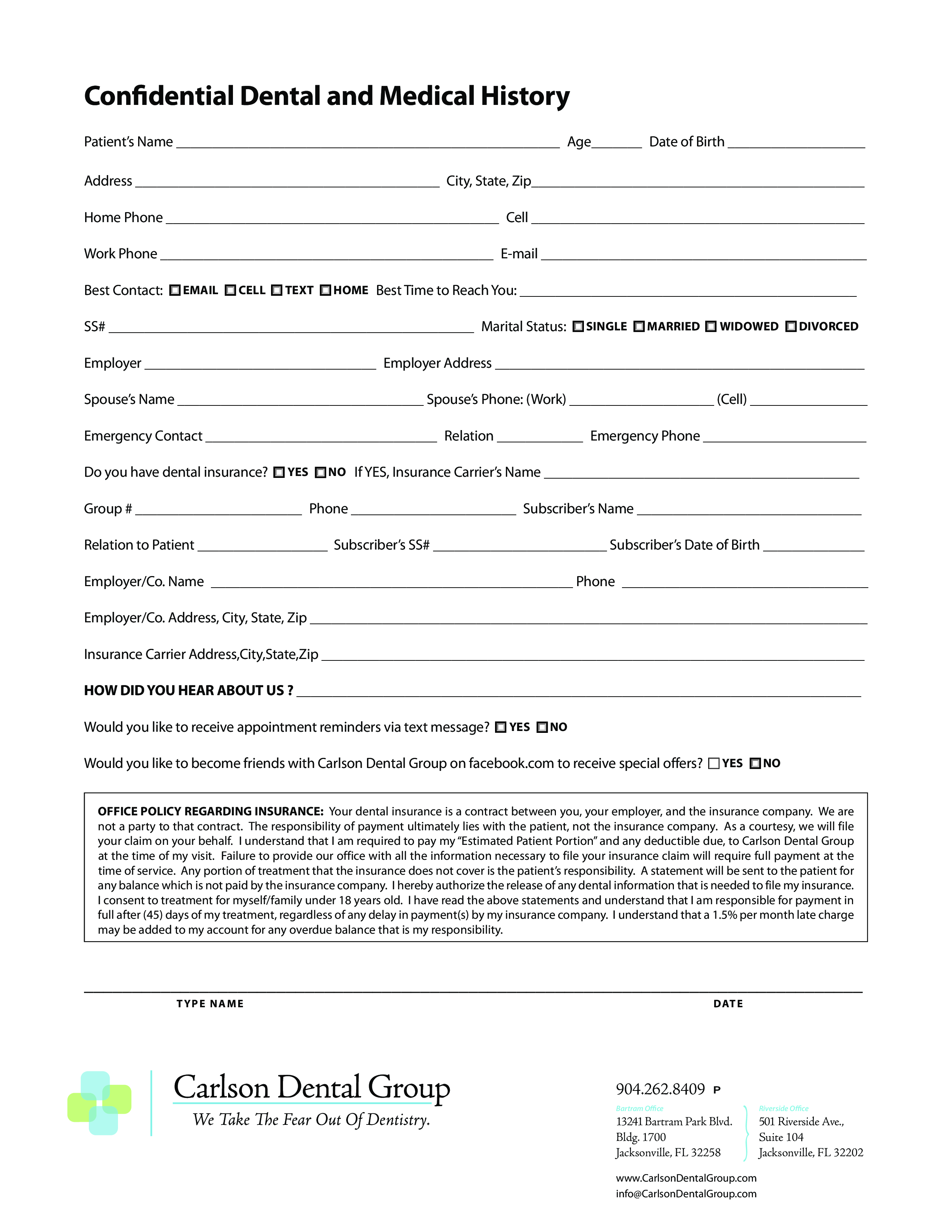
Prefered Method Of Contact (Select All That.
Date of your last dental exam: This office will collect, use and disclose information about you for the following purposes, including: • to deliver safe and efficient patient care and to. This form collects updated medical and dental history from patients.
To Ensure The Highest Quality Of Healthcare, We Ask That You Complete This Patient Update Form.
To ensure the highest quality of healthcare, we ask that you complete this patient update. What was done at that time? This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical. Complete it to ensure accurate healthcare and treatment.
Use The 2021 Edition Of The Ada Patient Dental And Medical Health History Information Form To Collect Pertinent Health Information And History From Your.
Your response to indicate if you have or have not had any of the following diseases or problems.